
Statin Liver Enzyme Interpreter
The real danger isn't usually the medication itself, but the reaction to the lab results. When patients see elevated enzymes, they often stop their medication out of fear. This creates a dangerous trade-off where the very real risk of a heart attack or stroke outweighs the theoretical risk of liver damage. Understanding what these enzymes actually are and why they move can help you stay on track with your cardiovascular health without unnecessary panic.
What Exactly Are "Elevated Liver Enzymes"?
When doctors talk about liver problems with statins, they are usually referring to ALT is alanine aminotransferase, an enzyme found primarily in the liver that leaks into the bloodstream when liver cells are damaged and AST is aspartate aminotransferase, an enzyme found in the liver and heart. Think of these enzymes like "smoke detectors." If they go off, it means something is happening inside the cell, but it doesn't always mean there is a raging fire.
In the context of Statins is a class of lipid-lowering medications that inhibit the enzyme HMG-CoA reductase to lower LDL cholesterol, a small percentage of patients (about 0.5% to 2.0%) experience an elevation where these enzymes climb above three times the upper limit of normal (ULN). For most, this is an asymptomatic event-meaning you feel completely fine, and the only way to know it's happening is through a blood test. Severe hepatotoxicity, which would actually compromise liver function, is exceptionally rare, occurring in fewer than 0.01% of users.
Why Do Statins Affect the Liver?
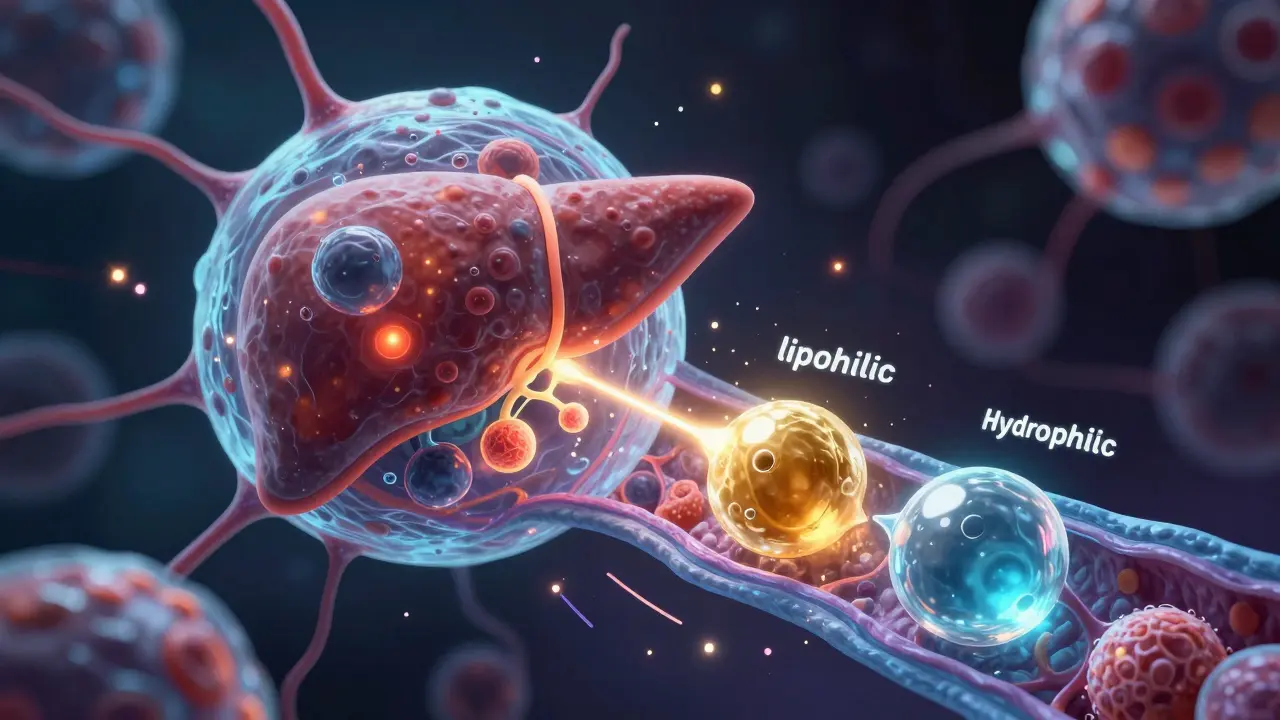
To understand why this happens, we have to look at the cellular level. Statins work by blocking cholesterol production, but they can also affect the mitochondria-the powerhouses of your cells. Research suggests that some statins can cause a reduction in membrane potential within the mitochondrial respiratory chain and increase the production of superoxide (reactive oxygen species). Essentially, it's a form of cellular stress.
Not all statins are created equal in this regard. There is a distinction between lipophilic and hydrophilic statins. Lipophilic statins, such as Simvastatin and Lovastatin, can easily cross cell membranes and have been shown to generate more reactive oxygen species than hydrophilic options like Pravastatin or Rosuvastatin. This is why some people find that switching to a hydrophilic statin resolves their enzyme issues entirely.
Additionally, genetics play a role. A specific variant in the SLCO1B1 gene, which helps transport statins into the liver, can make some individuals over three times more likely to experience these enzyme elevations. It's not a failure of the drug, but a quirk of how your specific body processes the chemistry.
How to Interpret Your Lab Results
If your doctor orders Liver Function Tests (LFTs) is blood tests that measure levels of proteins and enzymes to assess the health of the liver, don't let a single high number scare you. The clinical approach has shifted significantly over the last decade. The FDA updated its guidance in 2012, noting that routine, periodic monitoring of LFTs doesn't actually prevent serious liver injury because the injury is so rare and usually doesn't follow a predictable pattern.
| Enzyme Level | Typical Clinical Meaning | Standard Action Plan |
|---|---|---|
| Less than 3x ULN | Common, often transient, usually harmless | Continue statin; retest in 4-6 weeks |
| More than 3x ULN | Requires investigation | Temporary pause; investigate other causes; consider dose change |
| Severe/Acute (Jaundice) | Rare, serious liver injury | Immediate discontinuation and medical intervention |
It is also crucial to check for other culprits. If your ALT or AST is high, it might not be the statin at all. Common alternative causes include nonalcoholic fatty liver disease (NAFLD), alcohol consumption, or viral hepatitis. In some cases, patients with NAFLD actually show a lower incidence of statin-induced enzyme spikes than those without the condition, showing that the medication is generally safe even for those with existing liver issues.
Managing the Risks and Interaction
While the risk is low, you can lower it even further by being aware of drug interactions. Many statins are metabolized by the CYP3A4 enzyme system in the liver. If you take a medication that blocks this enzyme-like certain strong antibiotics (e.g., clarithromycin) or antifungal drugs-the levels of the statin in your blood can skyrocket. This increases the risk of both liver enzyme elevation and muscle pain.
For those who are high-risk, such as elderly patients over 75 with reduced kidney function, the chance of enzyme elevation is higher. In these cases, doctors might suggest a lower starting dose or a more frequent check-in during the first few months of therapy. The median onset for these elevations is usually around 12 weeks, though it can happen anywhere from one month to a year after starting the drug.
The Bigger Picture: Benefit vs. Risk
When you're staring at a lab report, it's easy to focus on the one number that is "out of range." But you have to weigh that against the "Number Needed to Treat." For primary prevention of cardiovascular events, the number of people you need to treat to prevent one major heart event is relatively small (around 39). Meanwhile, the number of people you need to treat before one person experiences a serious liver injury is huge-roughly 1,000.
Choosing to stop a statin because of a mild enzyme increase without consulting a doctor can be a mistake. Case studies have shown patients who stopped their therapy due to isolated ALT elevations and subsequently suffered cardiovascular events within 18 months. The goal is not "perfect" lab numbers, but a healthy heart and a long life.
Do I need regular liver tests while taking statins?
Current FDA guidelines suggest that routine periodic monitoring of liver function tests (LFTs) is not necessary for most patients. While a baseline test before starting the medication is recommended, follow-up tests are usually only required if you develop symptoms (like jaundice or dark urine) or if your initial baseline was already high.
What happens if my ALT levels are slightly high?
If your enzymes are elevated but less than three times the upper limit of normal, and you have no symptoms, most clinical guidelines recommend continuing the statin and re-testing in 4 to 6 weeks. Often, these levels normalize on their own without any change in medication.
Are some statins safer for the liver than others?
Generally, hydrophilic statins like pravastatin and rosuvastatin are associated with a lower risk of liver enzyme elevation compared to lipophilic statins like simvastatin and lovastatin. If a patient experiences liver-related issues with one type, switching to the other class often resolves the problem.
Can I take CoQ10 to protect my liver from statins?
Some phase II studies suggest that mitochondrial protectants like Coenzyme Q10 may reduce ALT elevations in some patients. However, while it may help with enzyme levels, there is not yet long-term data proving it improves cardiovascular outcomes or prevents serious liver injury.
Can I take statins if I already have fatty liver disease (NAFLD)?
Yes. Current clinical guidelines from the American Gastroenterological Association state that nonalcoholic fatty liver disease is not a contraindication to statin use. In fact, some data suggests patients with NAFLD may have a lower incidence of statin-induced enzyme spikes compared to the general population.
Next Steps for Patients
If you are concerned about your liver health while on a statin, start by reviewing your full medication list with your pharmacist to check for CYP3A4 inhibitors. If you receive a lab result with an "H" (High) next to your ALT or AST, don't panic or stop your meds immediately. Schedule a follow-up to determine if the elevation is transient or if a switch to a hydrophilic statin is a better fit for your genetics. Always prioritize the conversation about your total cardiovascular risk over an isolated lab value.